Treating and Managing COPD
How is chronic obstructive pulmonary disorder (COPD) Treated?
Treatment for COPD can vary from person to person.1 Goals of treatment include symptom control, reducing flare ups (exacerbations), improving quality of life, and reducing mortality.2 Treatment options may also help to slow the progression of the disease and improve your ability to stay active.1
Besides quitting smoking, medication is often one of the first treatment options for COPD; the type used depends on COPD severity or stage.1 Treatment may be combined with additional measures, such as pulmonary rehabilitation, oxygen, or surgery, as well as complimentary therapies like massage and acupuncture to help improve quality of life.1,2
Medications
COPD may be treated with a combination of quick relief (short-acting) and long-acting or controller medications.3,4 Quick relief medicine works fast to relax the airways; it should be taken when having symptoms.3 Alternatively, long-acting medicines are taken daily, reducing airway swelling and inflammation to prevent symptoms.3
Bronchodilators
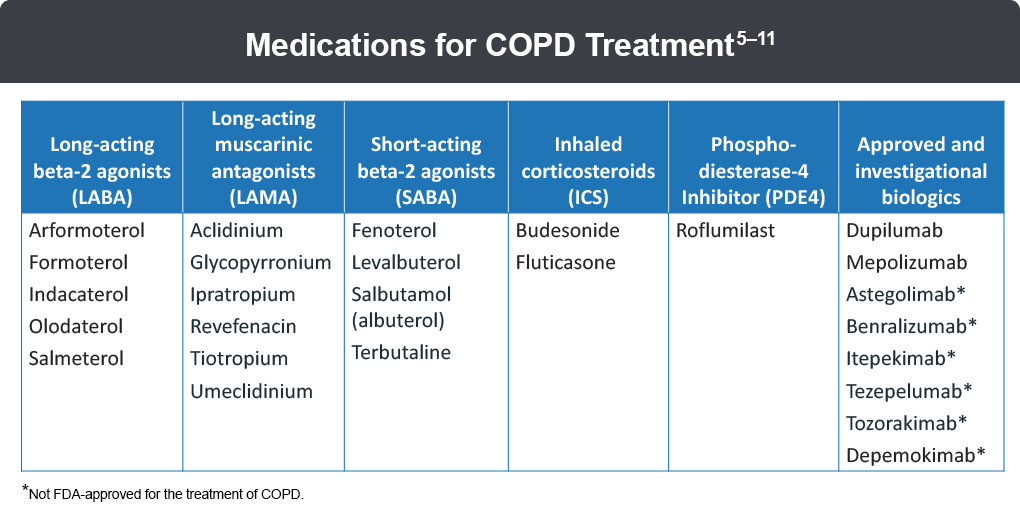
Bronchodilators relax the muscles around the airways; these can include short-acting or long-acting beta2-agonists.2,3 Short-acting beta-agonists (SABA) are used for immediate relief, but last only 4-6 hours; some SABAs include albuterol, metaproterenol, and levalbuterol. Long-acting beta-agonists (LABA) are used for daily maintenance therapy, lasting up to 12-24 hours; some LABAs include salmeterol, formoterol, arformoterol, olodaterol, and indacaterol.
Anticholinergics
Anticholinergics (or antimuscarinics) work by preventing muscles from tightening around the airways; this helps to keep the airways open and clear mucus from the lungs.2,3 Short-acting anticholinergics (SAMAs) work fast and are used as needed, whereas long-acting anticholinergics (LAMAs) are used as maintenance therapy.2,3 Some examples of LAMAs include glycopyrronium, tiotropium, ipratropium, aclidinium, umeclidinium, and revefenacin.3
Phosphodiesterase-4 inhibitors1
Phosphodiesterase-4 (PDE4) inhibitors block the breakdown of signaling molecule cyclic AMP, which can reduce inflammation. An example of a PDE4 inhibitor is roflumilast.
Anti-inflammatories1-3
Anti-inflammatory medications or inhaled corticosteroids (ICS) decrease inflammation, swelling, and mucus production inside the airways. ICS are often used in combination with LABAs or LAMAs and are recommended as combination therapy in moderate to severe COPD with increased risk of exacerbation, asthma and COPD overlap, or high blood eosinophil count.2,3 Some examples of ICS include fluticasone and budesonide.3
Corticosteroids (steroids) can also be taken as a pill, usually for a short duration when symptoms worsen.2,3 However, steroids can have serious side effects and should not be used long-term.2,3 Some examples of oral steroids include prednisone, prednisolone, and dexamethasone.3
Combination Therapy3
Combination therapy includes two or more medications within one inhaler or nebulizer treatment. Regimens combining therapy with 2 medications include ICS + LABA, LAMA + LABA, or SABA + SAMA. Triple therapy combines ICS with a LABA and LAMA and may be recommended in those with severe air flow limitation, more symptoms, blood eosinophil counts ≥100 cells/μL or with a history of COPD exacerbations.
Antibiotics3
Antibiotics may be used during a COPD exacerbation, which is often caused by bacterial or viral infections. Taking and finishing the antibiotic as prescribed is important in preventing infection reoccurrence and antibiotic resistance.
Biologic Therapy10-12
Understanding that COPD is caused by inflammation has resulted in the development of medications, called biologics, that can be used as an add-on therapy to a current regimen. Dupilumab and mepolizumab are two biologic agents approved for use in patients with uncontrolled COPD that is characterized by elevated blood eosinophils. Numerous clinical trials are studying the effectiveness and safety of other monoclonal antibodies including mepolizumab, benralizumab, itepekimab, astegolimab, tozorakimab, and tezepelumab.
References
- American Lung Association (ALA). Treating COPD. https://www.lung.org/lung-health-diseases/lung-disease-lookup/copd/treating
- Agarwal AK, Raja A, Brown BD, et al. Chronic obstructive pulmonary disease. Stat Pearls. 2023. Last update August 7, 2023. https://www.ncbi.nlm.nih.gov/books/NBK559281/
- American Lung Association (ALA). Understanding your COPD medications. https://www.lung.org/lung-health-diseases/lung-disease-lookup/copd/treating/copd-medications
- Agusti A, Celli B, Criner G, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Am J Respir Crit Care Med. 2023;207:819-837.
- Ari A. Jet, ultrasonic, and mesh nebulizers: An evaluation of nebulizers for better clinical outcomes Eur J Pulmonol. 2014;16:1-7.
- Kelsen SG, et al. Astegolimab (anti-ST2) efficacy and safety in adults with severe asthma: A randomized clinical trial. J Allergy Clin Immunol. 2021;148:790-798.
- Lazaar A, Miller B, Tabberer M, et al. Effect of the CXCR2 antagonist danirixin on symptoms and health status in COPD. Eur Respir J. 2018;52:1801020.
- Fahy W, Homayoun-Valiani F, Cahn A, et al. Nemiralisib in patients with an acute exacerbation of COPD: Placebo-controlled, dose-ranging study. Int J Chron Obstruct Pulmon Dis. 2021;16:1637-1646.
- Clinicaltrial.gov. Dose Finding Study of Nemiralisib (GSK2269557) in Subjects With an Acute Moderate or Severe Exacerbation of Chronic Obstructive Pulmonary Disease (COPD). https://www.clinicaltrials.gov/study/NCT03345407
- Dupixent (dupilumab). https://www.dupixent.com/copd.
- Nucala (mepolizumab). https://www.nucala.com/copd/.
- Rabe KF, Rennard S, Martinez FJ, et al. Targeting type 2 inflammation and epithelial alarmins in chronic obstructive pulmonary disease: A biologics outlook. Am J Respir Crit Care Med. 2023;208:395-405.
All URLs accessed March 10, 2025
12. Dupilumab (Dupixent®) Prescribing Information (PI) 2024 (www.regeneron.com/downloads/dupixent_fpi.pdf). Accessed 9/30/24.
